Article Text

Abstract
Objectives We compared intrapartum interventions and outcomes for mothers, neonates and children up to 16 years, for induction of labour (IOL) versus spontaneous labour onset in uncomplicated term pregnancies with live births.
Design We used population linked data from New South Wales, Australia (2001–2016) for healthy women giving birth at 37+0 to 41+6 weeks. Descriptive statistics and logistic regression were performed for intrapartum interventions, postnatal maternal and neonatal outcomes, and long-term child outcomes adjusted for maternal age, country of birth, socioeconomic status, parity and gestational age.
Results Of 474 652 included births, 69 397 (15%) had an IOL for non-medical reasons. Primiparous women with IOL versus spontaneous onset differed significantly for: spontaneous vaginal birth (42.7% vs 62.3%), instrumental birth (28.0% vs 23.9%%), intrapartum caesarean section (29.3% vs 13.8%), epidural (71.0% vs 41.3%), episiotomy (41.2% vs 30.5%) and postpartum haemorrhage (2.4% vs 1.5%). There was a similar trend in outcomes for multiparous women, except for caesarean section which was lower (5.3% vs 6.2%). For both groups, third and fourth degree perineal tears were lower overall in the IOL group: primiparous women (4.2% vs 4.9%), multiparous women (0.7% vs 1.2%), though overall vaginal repair was higher (89.3% vs 84.3%). Following induction, incidences of neonatal birth trauma, resuscitation and respiratory disorders were higher, as were admissions to hospital for infections (ear, nose, throat, respiratory and sepsis) up to 16 years. There was no difference in hospitalisation for asthma or eczema, or for neonatal death (0.06% vs 0.08%), or in total deaths up to 16 years.
Conclusion IOL for non-medical reasons was associated with higher birth interventions, particularly in primiparous women, and more adverse maternal, neonatal and child outcomes for most variables assessed. The size of effect varied by parity and gestational age, making these important considerations when informing women about the risks and benefits of IOL.
- obstetrics
- maternal medicine
- epidemiology
- neonatology
Data availability statement
No data are available. We do not have ethics approval to share data.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Size of data set and detailed variables utilised within the datasets.
Follow-up of children up to 16 years following the birth.
Examining induction of labour by parity and gestational age over 16 years.
Retrospective observational nature of the study design.
Inability to determine if stillbirths occurred antepartum or intrapartum.
Background
Rates of induction of labour (IOL) are rising globally,1 and around one in three women’s labours are now induced in some high-income countries.2 3 In Australia, in 2018, 45% of selected primiparous women (aged between 20 and 34 years, whose baby’s gestational age at birth was between 37 and 41 completed weeks, with a singleton baby in the vertex presentation) were induced.4 Overall the induction rate in the total Australian birthing population was 34%, almost a third increase in the last decade.4 Despite this there has been no significant reduction in the numbers of stillbirths or neonatal deaths in the last decade.4 A Cochrane systematic review of 30 randomised controlled trials (RCTs) examining maternal and perinatal outcomes associated with IOL compared with expectant management at or beyond term, found fewer perinatal deaths, fewer infants with Apgar score <5 at 7 min, fewer caesarean sections (CS), increased rate of operative vaginal births and no difference in perineal trauma, postpartum haemorrhage or length of maternal hospitalisation when labour is induced.5 The number needed to treat (NNT) in order to prevent one perinatal death was 426 in the Cochrane review.5 A more recent Cochrane review examining IOL at or beyond 37 weeks gestation also found a reduction in perinatal death (NNT 544), CS and neonatal intensive care unit (NICU) admission, with no increase in instrumental birth.6 However, based on a balance of all the risks and benefits considered, the current WHO guideline on labour induction only recommends the offer of IOL at or after 41 weeks of pregnancy.7
Two RCTs set up to assess the impact of routine IOL at around 39 weeks gestation on adverse neonatal consequences (including stillbirth) did not find a benefit for this primary outcome.8 9 Benefits were found in one RCT for primiparous women, in whom CS rates and some maternal outcomes, were improved in the IOL group.9 A meta-analysis including observational studies by the same author as the previously mentioned RCT,9 found a lower CS rate and improved neonatal outcomes.10
Two recent studies have addressed the issue of routine IOL for healthy women at 41 vs 42 weeks gestation.11 12 In the Dutch INDEX trial, a 1.4% absolute reduction was found in the rate of adverse perinatal outcomes in favour of IOL, although the rate of adverse outcomes were low in both groups (1.7% and 3.1%). No difference in CS was found (11% in both groups).11 The recent SWEPIS study, designed to address the question of routine IOL at 41 weeks compared with 42 in Sweden, was stopped because of an increased rate of stillbirth in the expectant arm (0% vs 0.4%).12 There were no significant differences in the composite perinatal outcome (2.4% vs 2.2%), mode of birth or maternal morbidity, other than endometritis, which was higher in the women who were induced.
In all these trials, significant numbers of women (70%–86%) declined participation,8 9 11 12 suggesting that those who took part might have had a different attitude to IOL than the large majority of women in the locality of the study population, raising questions about external validity.
Conflicting results come from cohort studies that describe what actually happens in routine practice. In a recent report from Denmark,13 birth outcomes were examined following a change in policy in 2011, which led to an offer of IOL for women between 41+3–41+5 weeks instead of 42 weeks. Examining 152 887 births between 2000–2010 and 2012–2016, the authors found no difference in stillbirths, perinatal deaths, low Apgar scores, CS and instrumental birth rate. However, over this period of time, rates of IOL, augmentation of labour, epidural analgesia and uterine rupture increased significantly.
Currently, there is disagreement about the level of risk that justifies routine IOL when it is associated with small absolute risk differences in perinatal mortality rates,14 potential adverse effects for women, and the variation in this and other outcomes across different studies and contexts, as noted above. No studies have examined longer term outcomes. Previously, as part of an examination of a range of intrapartum interventions, we noted associations between induction or augmentation of labour and short and long-term adverse neonatal outcomes.15 In the current study, we focused specifically on IOL in a low-risk population where no medical indication was identified, and we included follow-up data over a longer period of time.
The aim of our study was to examine short-term maternal and baby, and longer-term child health outcomes following IOL with no recorded medical indications, when compared with spontaneous onset of labour, in women with uncomplicated pregnancies who had not experienced a stillbirth.
Methods
Data were obtained from the Australian New South Wales (NSW) Centre for Health Record Linkage. The Centre utilises probabilistic data linkage techniques to merge data from the following datasets: Perinatal Data Collection (PDC); Admitted Patient Data Collection (APDC); NSW Registry of Birth Deaths and Marriages and the Australian Bureau of Statistics (Socio-economic Indexes for Areas, SEIFA). Probabilistic record linkage assigns ‘linkage weight’ to pairs of records.16 Records that match perfectly or nearly perfectly on first name, surname, date of birth and address have a high-linkage weight and records that match only on date of birth have a low-linkage weight.16 A false-positive rate of 0.3% of records has been reported.16 Studies have reported a tendency towards under-reporting of maternal prenatal medical conditions during linkage.17 18 The process of comparing the PDC and APDC data has increased the sensitivity and specificity for the purpose of identifying those women with medical complications.18 19
The committee agreed that consent could be waived due to the size of the dataset and retrospective nature of the data, and therefore, minimal risk of identification of individuals and the practical difficulties in obtaining consent.
Patient and public involvement
The data used for this study was routinely collected, deidentified and retrospective in nature. As a result, patients were not involved in the design and conduct of the study, choice of outcome measures or recruitment to the study.
Data set
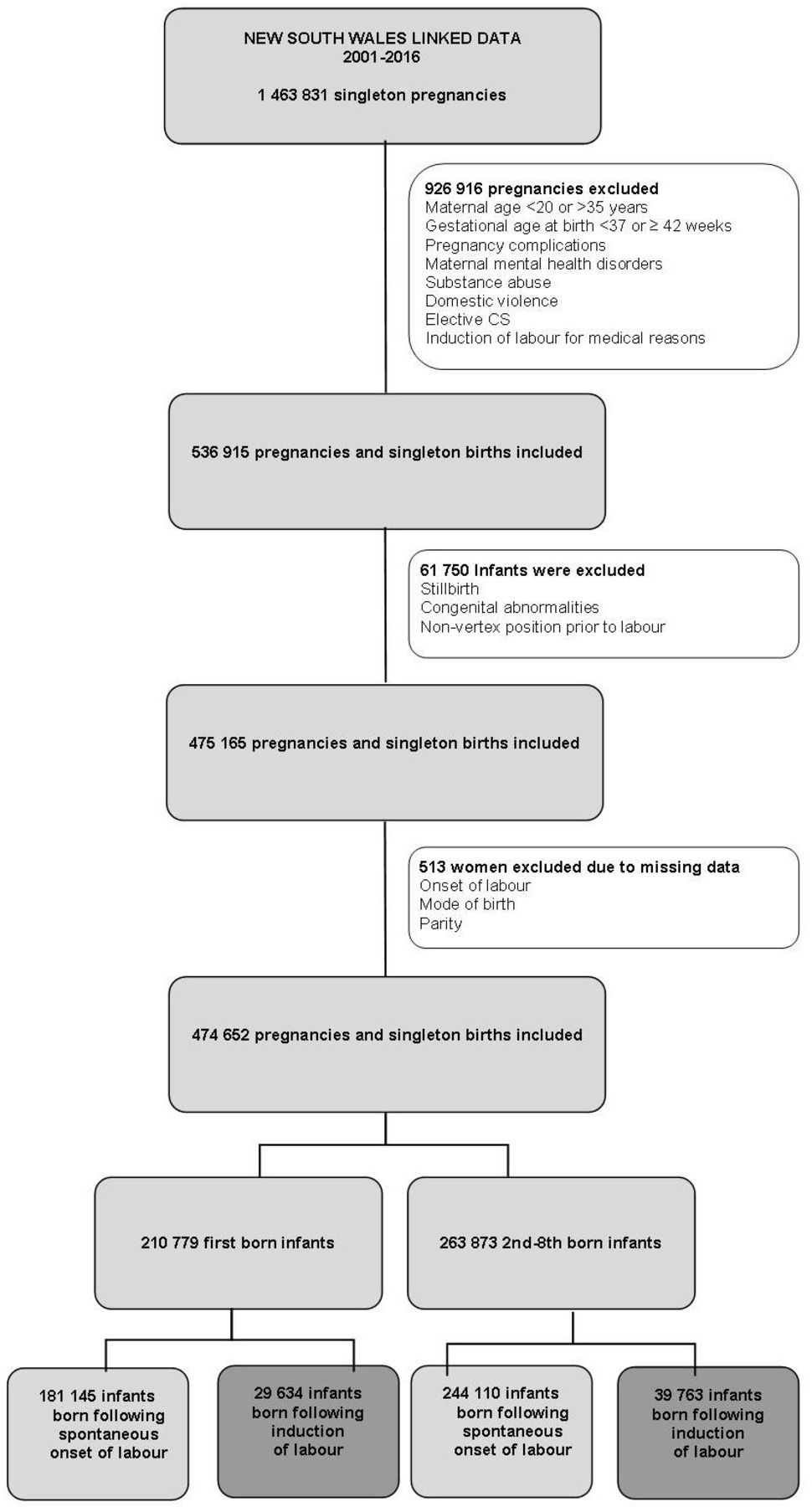
The datasets included routinely collected data on all women giving birth to a singleton infant between 1 January 2000 and 31 December 2016, with follow-up period for hospital admissions until 30 September 2017 (see figure 1). The information collected includes maternal demographic factors, pregnancy and labour characteristics, neonatal outcomes and adverse health outcomes of children (based on the International Statistical Classification of Diseases and Health Problems 10th Revision Australian Modification (ICD-10-AM).

Flow chart of study population. CS, caesarean sections.
As in our previous published study,15 we included women who were 20–35 years at the time of birth, and who gave birth between 37+0–41+6 weeks gestation to a singleton baby in cephalic presentation. Women were excluded if they had identified obstetric or medical risk factors during pregnancy or a record of substance abuse such as alcohol, drugs or smoking. For this study, we also excluded women with recorded social risk factors such as domestic violence, or recorded mental health disorders prior, during or after pregnancy. We also excluded women if they had an elective CS, or IOL for medical reasons (ie, diabetes, hypertensive disease, fetal distress, intrauterine fetal death, chorioamnionitis, blood group isoimmunisation and/or suspected intrauterine growth restriction).
Children with any congenital anomaly were excluded based on the ICD-10-AM codes, (Q0.0-Q99.9). Women were also excluded if they had a stillborn baby, as we were not able to determine if the baby was alive at the time of induction or onset of spontaneous labour. The primary aim of this study was not stillbirth, which has been the focus of several RCTs, but maternal and child health outcomes in a large low-risk population. Neonatal deaths were included in the birth outcomes but excluded from the long-term child health outcomes for follow-up purposes.
After applying all inclusion criteria, those with missing data on either type or gestation of labour onset, mode of birth or parity, were excluded from the analyses. If there were missing data on other variables such as country of birth, socioeconomic status, birth weight and interventions, these variables were indicated as system missing in the linked data file and subsequently excluded from the logistic regression models. Outcomes were reported separately for primiparous women and multiparous women, and for their neonates/children. Outcomes for each gestational week between 37 and 41 completed weeks were also reported in subanalyses.
Variables
Methods of induction included using synthetic hormones, artificial rupture of membranes and/or other methods such as the use of a Foley catheter. Spontaneous onset of labour was defined as commencing uterine contractions spontaneously. If the labour was also augmented in either group women were still included, as onset of labour was the focus and the study sought to mirror the clinical reality. The following intrapartum interventions and outcomes are reported herein: pharmacological pain medication (ie, nitrous oxide and opioids), epidural and/or combined caudal and spinal epidural for pain relief during labour, spontaneous vaginal birth, instrumental birth and emergency CS.
Short-term outcomes for infants included asphyxia, APGAR score <4 at 5 min, admission to special care nursery (SCN)/NICU, birth trauma including trauma to central or peripheral nervous system, scalp or skeleton or trauma causing intracranial laceration and haemorrhage; respiratory disorders (<28 days) including admissions in the perinatal period related to respiratory distress of the newborn or chronic respiratory disease; resuscitation, including resuscitation by suction and/or oxygen therapy, or major resuscitation including Intermittent Positive Pressure Ventilation (IPPV) by bag and mask, intubation and IPPV, external cardiac massage and ventilation and neonatal death <28 days. Children’s characteristics including gender, gestational age, birth weight and birth trauma were extracted from the PDC and APDC files.
The longer-term adverse health outcomes included asthma, ear nose and throat infections, eczema, respiratory infections (including admissions related to acute (obstructive) laryngitis, (bacterial) pneumonia. Other infections including bacterial sepsis, streptococcal sepsis) and mortality ≥28 days after birth were also extracted from the PDC file.
Short-term maternal health outcomes were derived from the PDC file and included postpartum haemorrhage for the total population. For women who gave birth vaginally the following perineal outcomes were derived from the PDC file: episiotomy, third/fourth degree tear and vaginal repair.
Other adverse health outcomes and other covariates with corresponding ICD-10-AM codes are presented in online supplemental appendix 1.
Supplemental material
Potential confounders for either women or children’s characteristics were selected from several data files. Maternal age and country of birth were extracted from the PDC.
SEIFA ranks areas in Australia according to relative socioeconomic advantage and disadvantage and education using women’s postal codes and defined as low (≤30 percentiles), medium (40–60 percentiles) or high (≥70 percentiles).
Data analyses
Baseline characteristics of all births were reported using descriptive statistics. Statistical differences in baseline characteristics in women and children in the two groups of interest (ie, women with either IOL or spontaneous onset of labour) were calculated with χ2 tests.
We used trend analyses to examine rates of IOL for non-medical reasons among primiparous women with uncomplicated pregnancies in the period 2001–2016.
For comparative analysis, we used spontaneous onset of labour as the reference group. Multinominal and multivariable logistic regression analyses were performed to examine the association between the exposure variable (IOL) and maternal and child health outcomes. In the total population, associations between IOL and short-term maternal and children’s outcomes were adjusted for maternal characteristics (ie, maternal age, country of birth, socioeconomic position, gestational age and parity). Next, associations were calculated separately for at term primiparous births (first birth) and at term multiparous births (subsequent births). All associations were adjusted for maternal age, country of birth, socioeconomic position and gestational age. Afterwards, associations were calculated individually for each completed gestational week and adjustments were made for maternal age, country of birth, socioeconomic position and parity.
Regarding the long-term health outcomes, adjustments were made for maternal characteristics (ie, maternal age, country of birth, socioeconomic, parity, gestational age) and children’s birth year, to control for the duration of the follow-up period.
All adjusted odds ratios (aORs) and the 99% CIs were calculated with the level of significance set at a p≤0.01. All statistical analyses were performed with SPSS Statistics V.25.0 (SPSS).
Results
The NSW linked data set contained data on 1 463 831 singleton pregnancies between 2000 and 2016. Rates of infant mortality were: 8236 stillbirths (0.6%), 3104 neonatal deaths (0.2%) and 3052 child deaths during the follow-up period (0.2%). In total 161 335 infants (11%) were diagnosed with some kind of congenital abnormality ranging from very minor to major.
A total of 989 179 pregnancies (67.6%) were excluded from the total NSW linked dataset, including 926 916 women who were excluded for the following reasons: medical or obstetric risk factors, for example, maternal physical, preterm birth (n=529 352); mental health disorders (n=98 550); substance abuse during pregnancy (eg, smoking or drug use) (n=83 795); social risk factors (eg, n=domestic violence) (n=4656); and birth related factors, (eg, elective CS, IOL for medical reasons) (n=210 563).
After this exclusion process was complete, 61 750 additional cases were excluded for reasons to do with the fetus/infant. This included a non-vertex position prior to labour (n=6482); congenital abnormalities (n=55 256); and stillbirth (n=12). Finally, 513 remaining women were excluded due to missing values.
Our final linked dataset included 474 652 women with singleton infants, of which 210 779 were first born and 263 873 were 2nd–8th born infants (no woman had more than eight babies) in their families (figure 1). There were 95 neonatal deaths up to 28 days and 411 children who died older than 28 days during the follow-up period.
Labour and birth characteristics
Among the 474 652 infants of the included population, 405 255 infants were born following a spontaneous labour (85%) and 69 397 (15%) were born after IOL without a recorded medical reason (table 1). In the IOL group, 45 370 (65.4%) women were induced with a combination of two methods, for example, artificial rupture of membranes and oxytocin/prostaglandin. The other women in the IOL group were induced with one method, for example, oxytocin/prostaglandin (n=16 974, 24.5%) or artificial rupture of membranes (n=6572, 9.5%) or other method such as Foley catheter (n=481, 0.6%).
Maternal, birth and infant characteristics of the included population, stratified for spontaneous onset of labour and induction of labour for non-medical reasons, New South Wales, Australia, 2001–2016 (N=474 652)
Compared with women with a spontaneous onset of labour, those with an induced labour were: older, more likely to be of Australian origin, of higher socioeconomic status, more likely to have an onset of labour between 40 and 41 weeks, and more likely to give birth to an infant with an average birth weight over rather than under 3500 g (table 1). In the total included population, women who were induced differed statistically significantly on all maternal, birth and child characteristics with all χ2 tests showing p≤0.001. These factors were, therefore, adjusted for in the analyses.
Over the 16-year time period, the rate of IOL doubled for 38 and 40 weeks of gestation, and the rate of IOL tripled for 37, 39 and 41 weeks of gestation (figure 2). The most marked increase was observed in induction rates at or around 37 weeks of gestation.

{kind=link}
{kind=link}
Change in rates of induction of labour among first time mothers with uncomplicated pregnancies associated with gestational age 2001–2017 NSW, Australia. NSW, New South Wales.
Short-term maternal health outcomes
In the included population, higher aORs were found for instrumental vaginal births, CS, episiotomy, vaginal repair and postpartum haemorrhage (PPH) among women who were induced versus those with spontaneous onset of labour. Fewer induced women had third or fourth degree tears compared with those with spontaneous onset (aOR 0.82 (99% CI 0.75 to 0.89) (table 2).
Proportions and associations of mode of birth outcomes, pain relief treatment and short-term maternal outcomes with induction of labour for non-medical reasons, New South Wales, Australia 2001–2016 (N=474 652)
Stratifying by parity
Primiparous women with IOL versus spontaneous onset differed significantly for: spontaneous vaginal birth (42.7% vs 62.3%), instrumental birth (28.0% vs 23.9%), intrapartum CS (29.3% vs 13.8%), epidural (71% vs 41.3%), episiotomy (41.2% vs 30.5%) and PPH (2.4% vs 1.5%). There was a similar trend in outcomes for multiparous women, except for CS which was lower (5.3% vs 6.2%). For both groups, third and fourth degree tears were lower overall in the IOL group: primiparous women (4.2% vs 4.9%); multiparous women (0.7% vs 1.2%)—though overall vaginal repair was higher (89.3% vs 84.3%).
Stratifying by gestational age
When stratifying data by gestational age, the patterns changed (table 3). For all gestational ages, primiparous women who were induced had higher aORs for vaginal instrumental births, CS, pharmacological pain medication, epidural/spinal anaesthesia, episiotomy, vaginal repair and PPH. The statistically significant benefit to primiparous women was of a lower incidence of third and fourth degree tears for those induced at between 40 and 41 weeks gestation, though this group still had a higher rate of episiotomy and vaginal repair than primiparous women who were not induced. For multiparous women who had an induced birth, statistically significantly higher aORs were found for instrumental vaginal birth, episiotomy and PPH for all gestational ages apart from 37 weeks, where no significant differences were noted. AORs for pharmacological pain relief and epidural pain relief were higher for women with IOL at all gestations. For multigravida women with induced labours, the aOR for CS were lower at 37, 38 and 39 weeks and higher at 40 and 41 weeks. For pharmacological pain medication in general, and epidural or spinal analgesia specifically, aOR’s were higher for all gestational ages. For third or fourth degree tear there was no significant difference for multigravida women at 37–38 weeks or 41–42 weeks gestation, but the aORs were lower at 38, 39 or 40 weeks gestation. Multigravid women who were induced had higher aORs for vaginal repair than those who were not induced, at all gestations except 37–38 weeks.
Proportions and associations of mode of birth outcomes, pain relief treatment and short–term maternal outcomes with induction of labour for non-medical reasons, stratified for gestational age groups 37–41 weeks, New South Wales, Australia 2001–2016 (N=474 652)
Short-term and long-term infant health outcomes
Infant short-term outcomes
In the included population, higher aORs were found for admission to NICU/SCN, asphyxia, birth trauma, any resuscitation, major resuscitation (IPPV by bag and mask, intubation and IPPV, external cardiac massage and ventilation), and respiratory disorders among women who were induced vs those with spontaneous onset of labour. No associations were found between induction for non-medical reasons and Apgar score <4 and neonatal death (table 4). These findings did not differ by parity, except for the association between IOL and NICU/SCN admissions, that became non-significant. There was no statistically significant difference in neonatal death <28 days postpartum and child mortality >28 days and up to 16 years of age.
Proportions and associations of short and long-term infant outcomes associated with induction of labour for non-medical reasons, New South Wales, Australia 2001–2016 (N=474 652)
Stratifying by gestational age
When stratifying the analyses by gestational age for the population as a whole the predominance of adverse short-term infant outcomes tended to be among early term births (ie, 37 and 38 weeks), including 39–40 weeks for birth trauma, all forms of resuscitation and respiratory disorders, except for major resuscitation which was greater for neonates after IOL in all gestational weeks and Apgar score <4, which was not significantly different in any gestational week (table 5). Associations between IOL and neonatal death by gestational age could not be calculated due to the low numbers that occurred in this low risk population(n=95).
Proportions and associations of short-term infant outcomes with induction of labour for non-medical reasons, stratified for gestational age groups 37–41 weeks, New South Wales, Australia 2001–2016 (n=4 74 652)
Long-term child health outcomes up to 16 years
Among the 474 146 children who were alive during the study period and were born to women who were induced for non-medical reasons, higher aORs were found for hospitalisation for all types of infection (ie, ear, nose and throat, respiratory infections and other infections) compared with those born following a spontaneous onset of labour. When stratifying by gestational age, significantly higher aORs were observed for hospital admission for respiratory infections by all gestational ages; and for ear nose and throat infections for those born after IOL at between 38 and 41 weeks. Overall risk of hospital admission for infections was significantly higher for those born at between 39 and 41 weeks gestation by IOL (table 6).
Proportions and associations of long-term infants outcomes with induction of labour for non-medical reasons, stratified for gestational age groups (37–41 weeks), New South Wales, Australia 2001–2016 (n=4 74 146)
For the total population, there were no associations found between IOL for non-medical reasons and the long-term outcomes of hospitalisation for asthma, eczema and mortality ≥28 days after birth (table 4). There was no change in this finding when stratifying the analyses for gestational age (table 6).
Discussion
This large linked data population study found that the rate of IOL with no medical indication for women with uncomplicated pregnancies tripled at some gestational ages between 2001 and 2016. Women with uncomplicated pregnancies who had their labour induced had higher rates of epidural/spinal analgesia, CS (except for multiparous women induced at between 37 and 40 weeks gestation), instrumental birth, episiotomy and PPH than women with a similar risk profile who went into labour spontaneously. Between birth and 16 years of age, and controlled for year of birth, their children had higher odds of birth asphyxia, birth trauma, respiratory disorders, major resuscitation at birth and hospitalisation for infection. In this study, only hospital admissions were examined and hence more serious illnesses. Though this risk varied by gestational age of labour onset, there was no gestational age for which any of these risks were significantly lower for those born after IOL when compared with those born after spontaneous labour onset.
For two major outcomes the adjusted odds were lower for some women following IOL at specific gestational ages. These were third/fourth degree tear, for multiparous women induced between 38 and 41 weeks gestation, and for nulliparous women induced at 40–41 weeks gestation; and CS for multiparous women induced between 37+0 and 39+6 weeks. However, for those who started labour between 40+0 and 41+6 weeks, the CS rate was higher among multiparous women who had an induced labour.
Strengths and limitations
We included infants born at term after a healthy pregnancy in NSW, Australia between 2001 and 2016. Their hospital admissions were followed up in the period 2001–2017. As far as we are aware, this is the largest ever whole-population study with a focus on mode of labour onset, and with linked data follow-up for nearly two decades. Using population- based linked data allowed us to compare rare and longer-term outcomes which is not possible in RCTs due to the limited sample sizes. However, we were restricted to available variables, and a limited ability to verify the accuracy of registration data.
We could not analyse stillbirth separately as an outcome as it was unclear whether IOL was undertaken for stillbirth prior to labour onset, or if the stillbirth occurred after labour had commenced. A similar rationale was applied to exclude stillbirths in a recent large scale epidemiological analysis of birth complications by parity and maternal risk status.20 We also did not have access to neonatal umbilical pH or Lactate in the population data set we analysed and this is not done routinely at every birth in Australia. Long-term maternal morbidity was also not examined and needs to be addressed in future research.
We cannot establish causality in our study. Although we adjusted for a range of confounders, our associations could be affected by unmeasured factors that could influence short and longer-term outcomes, including the lack of consistent data on antibiotic use, method of infant feeding, paternal or familial characteristics, ethnic group or environmental factors. However, given the large scale of the study, and the size of the differences we found for some variables, we believe it is critically important that the findings are taken into account in information given to women about the potential advantages and disadvantages of IOL, and when designing future prospective studies in this field.
We were not able to report on visits to general practitioners in the follow-up period for maternal and children’s outcomes. However, it is likely that a visit to hospitals with specific conditions is an indicator for more severe disease than a visit for community-based healthcare, so our findings on the longer term impact of IOL for children are likely to reflect serious outcomes that are important to families and to the health system.
The results of this study could have been different if it had been conducted prospectively, based on intention to treat. It is also possible some of the women induced without medical reasons identified may have had medical indications for their induction but were misclassified in their electronic patient files. Women with a stronger preference for physiological birth may also have not chosen, or agreed to IOL, and they may be more likely to pursue a normal labour and birth. However, the data sources have a good track record of accuracy, so we do not believe these errors are likely to be large, or that they would have significantly influenced the direction of effect of the outcomes.
Interpretation
This study raised important questions as to why the short-term results are so different from the RCTs discussed at the beginning of the paper. For example, CS rates were around three times higher for primiparous women at all gestational ages of labour onset, in direct contrast to the outcomes from a recent RCT.9 This may be due to selection bias within our study. Alternatively, it could be a function of non-representative study populations in RCTs. In all the recent RCTs examining the question of IOL versus spontaneous onset of labour, significant numbers of women (70%–86%) declined participation8 9 11 12 suggesting that those who took part might have had a different attitude to IOL than the majority of women in the local population, raising questions about external validity of the trial results. This was one of the reasons why we wanted to take a whole population approach in our study, to reflect the actual experience of hundreds of thousands of women and their children, over an extended time period. Our data accord with other whole population, longer term observational studies, such as that reported recently from Denmark.12
For some multiparous women, two outcomes were improved following IOL when compared with spontaneous labour onset. Emergency CS rates were lower following induction in multiparous women at 37–40 weeks gestation; however, instrumental birth rates were higher for those who had IOL between 38 and 42 weeks gestation. The long-term impact of more instrumental birth on pelvic floor damage needs to be considered,21 but we did not have the data on this.
The lower rates of third and fourth degree perineal trauma following IOL, mostly for multiparous women, is intriguing, as they had higher rates of vaginal birth, episiotomy, and instrumental birth, all of which have been cited as risk factors for severe perineal trauma.22 Both primigravid and multigravida women with induced labours at all gestational ages had higher rates of vaginal repair, except at 37–38 weeks when no differences were evident. The longer-term benefits of reduced rates of third and fourth degree tears need to be followed up in future longitudinal studies, as well as the benefits of intact perinea. It is possible that some third and fourth degree tears were not reported when an episiotomy was, thus leading to a lower rate. Australian data is recognisably unreliable in this area given 25% of women have care from private obstetricians and the under-reporting of severe perineal tears in private hospitals has been raised previously.22 We did not find any differences in neonatal outcome in our study, but we did not examine the impact on intrapartum stillbirth, and there is evidence on reduced adverse perinatal outcomes (and on some maternal outcomes, such as pre-eclampsia) in the current trial data.5 6Our data, therefore, need to be balanced with these findings from RCTs.
It is widely agreed that, on the basis of ‘first do no harm’, interventions should not be undertaken for women with uncomplicated pregnancy, labour and childbirth unless there is clear evidence of benefit, either at the population or the individual level. There is an ongoing debate about the appropriate indications for, and timing of, IOL in the absence of any indication apart from gestation.14 23 WHO has advised against IOL without medical indication before 41 weeks gestation,7 and the 2016 Lancet series on Maternal Health concluded that IOL was one of the interventions done ‘too much too soon’ in many settings.1 There is also rising particular concern about potential neurological impacts from iatrogenic early birth.24
Importantly women have mixed responses to IOL and this needs to be better understood. A recent review of 10 qualitative studies found women did not feel involved in decision making regarding IOL and they were unprepared for many of the aspects of the process.25 In a Swedish cohort study, women who were induced more often used epidurals for pain relief and were less satisfied.26 This contrasts with findings that there is no difference in need for labour pain relief, or perception of pain reported in one of the RCTs discussed above,9 while others do not report this outcome. Another recent scoping review studied both women’s and clinicians’ experiences of care and decision making regarding IOL and found women’s expectations and preferences are often unmet and decision making largely informed by clinicians’ attitudes towards indications for IOL, rather than involving women in shared decision making.27 There is also widespread unexplained variation in clinical practice guidelines for IOL.28
Considerations for future research
There is an urgent need to understand why the observational data on IOL are consistently at odds with the findings from RCTs. More large whole population observational studies from different contexts would help with constructing accurate locally relevant information for maternity care providers and for women, especially if these studies set a priori criteria for adjustments, and for subgroup analysis, with all concerned stakeholders. It is also important to examine the influence of both service users and service providers prior values and beliefs on labour onset, and the organisational contexts and maternity care ethos in which both RCTs and observational studies are conducted.
Our study did not include data on longer-term clinical and psychological impacts for women. The evidence on women’s experiences of IOL when there is no medical indication is mixed to date and has not been modelled by parity and other factors, such as women’s choices for or against IOL in the absence of medical indications. The choices women make in subsequent pregnancies following an experience of IOL also need to be explored further, with emerging evidence that some women seek to have homebirths and freebirth in order to avoid perceived pressure to accept IOL in hospital.29 The psychological impacts for women whose labours are induced compared with those that are not need further exploration, especially into the long term.30–32 Health economic analysis should be considered, including an assessment of opportunity costs in relation to availability of resources for women and neonates with higher levels of risk if women at low risk are routinely offered induction at ever lower gestations.1 14 33 Our findings indicate that any future research in this area should account for parity, gestational age and longer-term outcomes, as a basis for informing women about individualised risks and benefits of different labour-onset options.
Conclusion
IOL can be lifesaving. However, our data suggest that, for women who do not have a medical indication for labour induction at or near term, there could be increased rates of intrapartum interventions and adverse outcomes in the short term for mother and neonate, and of hospitalisation for infection in the longer term for children. We did not find any benefits of IOL for neonates, at any term gestation of labour onset. The size of effect for most variables we assessed varied by parity and gestational age, making these important considerations to focus on in future studies. When IOL is requested by women or offered to them without a specific medical indication (other than gestational age), these short-term and long-term outcomes should be included in the information discussed with them. Women’s views and experiences as well as their long-term maternal outcomes should be considered in future research.
Data availability statement
No data are available. We do not have ethics approval to share data.
Ethics statements
Ethics approval
The study was approved by the Ethics Committee of the NSW Population and Health Services Research Committee (HREC/10/CIPHS/96).
Acknowledgments
We would like to thank the NSW for Health Record Linkage (CHeReL) for Linkage of the datasets.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @hannahdahlen
Contributors HGD formulated the study and wrote the paper with LP, CT, SD and AdJ. LP analysed the data. CT and AS-S checked data and provided statistical advice. ST and MT provided advice on the manuscript and neonatal outcomes. AB provided obstetric advice.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.